


















Desmoids of the Shoulder and Bilateral Breasts in the absence of FAP or Gardner’s Syndrome: A Case Report and Review of the Literature
Abstract
Desmoid tumors constitute 0.02% to 0.03% of all tumors. Consequently, few case reports exist for breast desmoids, even fewer identifying bilateral disease. We present a case report of a patient with bilateral breast desmoids and shoulder desmoid without evidence of FAP or Gardner’s syndrome. This case report explores the clinical, radiographic, pathological, and treatment elements for desmoid tumors as well as a review of the literature.
Introduction
Desmoid tumors account for less than one-tenth of one percent of all tumors.1 Few case reports and even fewer series pertaining to breast desmoids exist in the literature.2-22 Several large case series did not contain any bilateral tumors.19, 21 These tumors typically present in younger women in their third to fifth decades of life,20-24 although there are case reports in males.25-27 In the very few instances of bilateral breast involvement cited in the literature, most of these tumors are synchronous not metachronous.24
The tumors typically present as a lump in a patient’s breast without any associated discharge or pain. The tumors typically range in size from 1 to 10 cm with a mean in most series of 3 cm.24 When detected by mammography, these tumors are stellate in their appearance with the peculiar absence of calcifications, a distinguishing feature between desmoids and breast carcinoma.2, 6-9, 25 The sensitivity of detection by mammogram is relatively poor, and ultrasound and MRI are frequently used to assist in the imaging and diagnostic process.24 The sensitivity of these two tests in several series is close to 100%.24 In general, MRI in the case of desmoids is useful because many of these tumors do not arise out of the parenchyma but from the chest wall.28 Fine needle aspirate and even core needle biopsy can yield nondiagnostic biopsies, and excisional biopsy is frequently required.24 Histopathology is of paramount importance in differentiating this disease from carcinoma, as desmoids may appear much like carcinoma on imaging and gross evaluation.25
Desmoid or fibromatosis is characterized histologically by a bland proliferation of spindle cells with scant cytoplasm.29 Long fascicles of myofibroblast activity with increased cellularity at the periphery as well as few mitoses and mild nuclear atypia are typical findings. B-catenin, vimentin, actin, and rarely desmin are positive, while CD34 is negative.30
Once a diagnosis is made, these tumors should be resected aggressively with lumpectomy with clear margins up to 3 cm or with mastectomy. Though these tumors have not demonstrated metastatic potential they are locally aggressive with a recurrence rate around 30%.8, 20, 24 Though these tumors arise de novo, a surgical procedure may initiate the disease process, and several case reports after breast augmentation have been documented.5, 11, 31-34
Case presentation
A 29 year old female palpated a mass in her right breast on self breast exam approximately 2 weeks prior to presentation to Kansas University Medical Center on 6/25/2009. The patient felt as though the mass was growing and as such scheduled an appointment for consultation and evaluation.
The patient had a history of fibrous breasts with biopsy performed in 2001 with no concerning pathology identified. She was an otherwise healthy female with no prior surgical or medical history. She had been taking estradiol tabs at the time of her consultation. Her family history included a maternal great grandmother who succumbed to breast cancer in her sixth decade. She had no other family history of breast cancer or additional cancers. Finally, she was a nonsmoker.
On physical exam, her right breast revealed a 3 x 3 cm nodular mass at the one o’clock position. Her left breast revealed a 3 x 3 cm nodular mass at the 11 o’clock position. She had no palpable lymphadenopathy. She was imaged that day, 6/25/09, with mammograms and ultrasound. Additionally, ultrasound guided biopsies of both breasts were performed. The following day, breast MRI was obtained. Mammography confirmed 3 cm masses bilaterally. These were speculated noncalcified masses highly suggestive of malignancy. Ultrasound showed 2 to 3 cm masses bilaterally without evidence of axillary disease. MRI of the breasts showed minimally suspicious uptake in a diffuse distribution in the right superomedial quadrant. The uptake was indeterminate and nonspecific. Very little abnormal uptake was seen in the left breast. Ultrasound guided needle biopsy was benign and discordant. As such, excisional biopsy was scheduled.
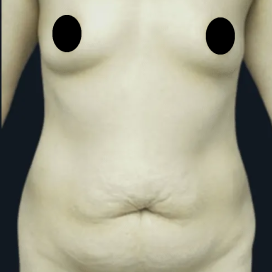
Her initial surgery of bilateral lumpectomies was performed on 7/9/2009 (see Figure 1).
Figure 1: s/p bilateral lumpectomies on 7/9/2009.
Pathology revealed bilateral desmoid tumors. Immunohistochemical stains showed the tumor to be Desmin(-), CD34(-), and S100 (-). The lumpectomy specimen on the right measured 3.2 cm x 2.6 cm x 1.6 cm. Sectioning revealed a 1.7 cm x 1.2 cm x 1.0 cm white ovoid mass. The left lumpectomy specimen was 2.7 cm x 2.5 cm x 1.8 cm and revealed a similar appearing lesion measuring 1.8 cm x 1.4 cm x 1.3 cm. In both lumpectomy specimens, the lesion extended to the resection margins, including the deep, superficial, superior, and inferior margins.
After informing the patient of the nature of the tumor, the patient opted for bilateral mastectomy and bilateral tissue expander placement with Alloderm sling. Given the tissue diagnosis of desmoid tumor, a previous excision site for BCC on her left shoulder was biopsied, given a somewhat uneven contour to the area.
On 9/9/09, bilateral mastectomies were performed. The pectoralis muscle at the deep margin was also biopsied. The mastectomy specimens captured the desmoid tumors in their entirety with at least 2 cm borders clear in every dimension. There was no invasion into the muscle or chest wall.
Of note and interest, the previous scar of the left shoulder showed a proliferation of bland spindle cells consistent with fibromatosis (desmoid tumor) involving the 6, 9, and 12 o’clock margins. The patient elected to undergo radiation of this area with surgical resection to follow.
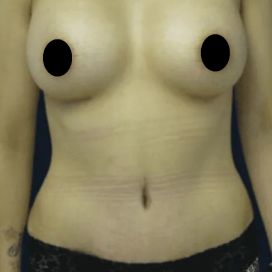
On 1/11/2010, the patient underwent TE removal and implant placement with capsulotomy and excision of shoulder lesion (see Figure 2).
Figure 2: s/p bilateral mastectomies with TE/implant reconstruction and left shoulder lesion excision
During this operation, the skin at the mastectomy sites was biopsied and showed bland, fibrosing spindle cell proliferation associated with foreign body giant cell reaction, suggestive of scar. Similarly, the excision of the shoulder lesion appeared complete. However, discussion with pathology revealed that distinguishing between the fibrosis of scarring and residual fibromatosis can be exceedingly challenging on histologic grounds. Pathology favored scar rather than residual fibromatosis due to lack of broad, sweeping fascicles, the presence of intermixed foreign body giant cell reaction and the lack of definitive nuclear staining with the beta catenin immunostain. However, they recommended close clinical follow-up.
Of note, a portion of the Alloderm and skin from the right breast were sent as well and revealed fibrosis and foreign body giant cell reaction, compatible with scar. There may be a role for Alloderm in these rare situations as it offers a barrier between adjacent areas of scar and may make pathological diagnosis of margins less difficult in desmoid tumors.
The patient has been closely followed closely since her surgery on 1/11/2010. For completeness given the syndromic nature of desmoid variants, the patient underwent additional workup including colonoscopy and negative mucosal biopsies despite lack of family history. The patient did not undergo any additional postoperative radiation to any of the involved areas.
In June 2010, the patient had MRI of bilateral breasts, which revealed postsurgical changes of bilateral mastectomy with implant reconstruction. No abnormal enhancement or discrete mass was observed to
suggest residual or recurrent tumor. An MRI of the left upper extremity showed no nodular soft tissue enhancement to suggest residual or recurrent desmoid.
In September 2010, patient was noted to have an additional mass at the site of the previous shoulder excision. She underwent MRI evaluation, which revealed no obvious evidence of recurrent disease. However, due to the nature of the disease process, the area was re-excised and closed. Follow-up pathology revealed no evidence of recurrent desmoid tumor.
Discussion
Desmoid tumors of the breast typically present in younger women as in the case presented above. However, she presented bilaterally, accounting for a small minority of the cases.20 Our patient’s additional desmoid of the shoulder creates a unique clinical picture for the literature. Desmoid tumors can involve the chest wall in approximately 50% of cases, although our patient’s disease was confined to the parenchyma.25 Thus, her probability of recurrence is estimated to be around 30%. The risk of recurrence may be as high as 57% when the chest wall is involved.8 Local recurrence should be radically excised, and. radiotherapy can be considered if radical excision of would result in unacceptable functional loss.35 Radiotherapy has also been used for positive margin tumors following excision.35
There is a higher risk of recurrence in the first 3 years after primary excision, and some have suggested that breast reconstruction may be best delayed for this period.8, 14, 35, 36 There is an additional case report of desmoids occurring after breast reconstruction .13 Conversely, other authors have demonstrated effective immediate breast reconstruction without recurrence, though the numbers are few.37
Although our patient does not appear to have disease consistent with Gardner’s syndrome or FAP, surveillance is always indicated.26, 34, 38, 39 Colonoscopy should be performed in these instances.38
Conclusions
Desmoid tumors of the breast remain a perplexing issue in surgical management of the disease as local recurrence despite aggressive treatment still remains high. The rarity of the disease prevents appropriate randomization and determination of the benefits of radiation, chemotherapy, and other therapies. The case presented in this paper highlights the need for meticulous preoperative and diagnostic workup in these patients, as when one desmoid is identified, many may exist even in the absence of a syndromic or familial disease association. One can only speculate as to the appropriateness of immediate or delayed reconstruction in these cases as only a handful of these cases after reconstruction have been described. Additionally, with the advent of new biologics such as Alloderm, early recurrence versus scar formation may be more accurately ascertained.
Article 1: The Role of Telemedicine in the Management of the Cosmetic Surgery Patient
Article 2: Breast Implant Reconstruction after Radiation
Article 3: Breast Reconstruction after Mastectomy
Article 4: Protocol for the Management of Keloid Scars
Article 5: Melanoma and the Role of Sentinel Lymph Node Biopsy
Article 6: Desmoid tumors of Bilateral Breasts
Article 7: The Role of the Paramedian Incision
Come to Hughes Plastic Surgery in Los Angeles and Beverly Hills. You will be glad that you did.
